
Glioblastoma Multiforme (GBM) remains one of the most aggressive and treatment-resistant brain cancers, presenting major challenges in oncology and neurobiology. As researchers continue to explore next-generation therapies, including NK cell immunotherapy and precision medicine approaches, advanced human-relevant models such as cerebral organoids are transforming the way GBM progression, invasion, and therapeutic response are studied. This article explores the biological complexity of GBM, emerging therapeutic strategies, and the growing role of human cerebral organoid platforms in translational glioblastoma research.
In This Article
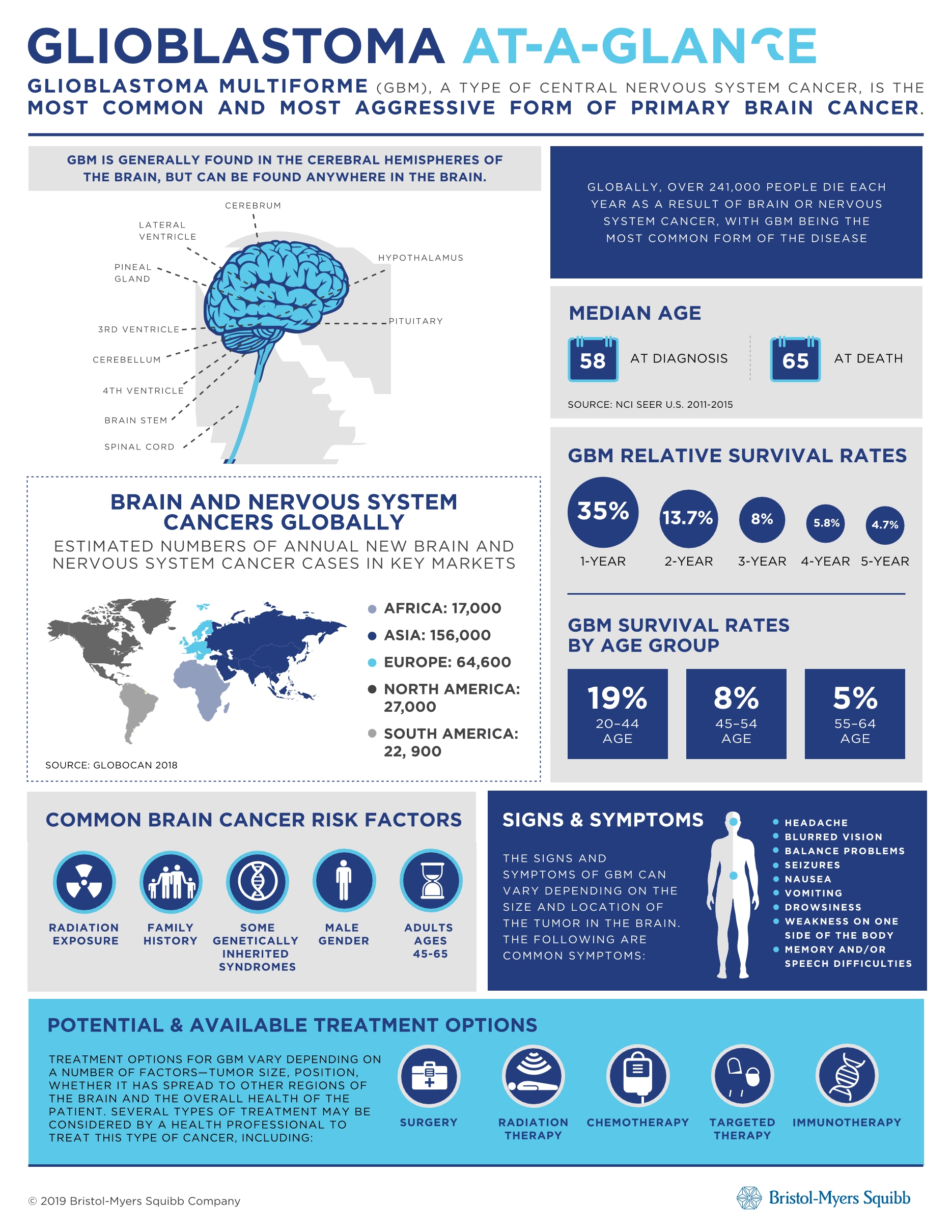
Understanding Glioblastoma Multiforme (GBM)
Glioblastoma Multiforme (GBM) is the most aggressive and common primary malignant brain tumor in adults. Classified as a Grade IV astrocytoma by the World Health Organization (WHO), GBM is characterized by rapid growth, diffuse infiltration into surrounding brain tissue, high cellular heterogeneity, extensive angiogenesis, and strong resistance to therapy (Wen & Kesari, 2008; Ostrom et al., 2023).
Despite decades of research and advances in neuro-oncology, GBM remains one of the deadliest solid tumors, with a median overall survival of approximately 12–15 months after diagnosis. The five-year survival rate remains below 10%, highlighting the urgent need for more effective treatment strategies and human-relevant preclinical models (Stupp et al., 2005; Ostrom et al., 2023).
Key Biological Features of GBM
- Highly invasive growth patterns
- Extensive intratumoral heterogeneity
- Presence of glioma stem-like cells (GSCs)
- Hypoxic and immunosuppressive tumor microenvironment (TME)
- High recurrence rates after treatment
- Blood-brain barrier (BBB) limiting drug delivery
GBM commonly involves alterations in genes and signaling pathways such as:
- EGFR amplification
- TP53 mutations
- PTEN loss
- IDH1/IDH2 mutations (in subsets)
- MGMT promoter methylation
- PI3K/AKT/mTOR signaling dysregulation
These molecular complexities contribute to therapeutic resistance and disease recurrence.
Read More:
Modeling Brain Diseases With Human Cerebral Organoids
Advancing Parkinson’s disease research with human midbrain organoids
Challenges in Glioblastoma Treatment
1. Tumor Heterogeneity
GBM tumors contain diverse populations of cancer cells with distinct genetic and phenotypic profiles. Even within the same patient, multiple subclones may coexist, each responding differently to treatment.
This heterogeneity complicates:
- Drug development
- Biomarker discovery
- Precision medicine approaches
- Long-term therapeutic efficacy
2. Invasive Nature of GBM
Unlike many solid tumors that form well-defined masses, GBM cells infiltrate deeply into healthy brain tissue. Surgical resection cannot completely remove these invasive cells, leading to recurrence.
3. Blood-Brain Barrier (BBB)
The BBB restricts the penetration of many therapeutic agents into the brain. Even promising anticancer compounds may fail clinically due to insufficient brain delivery (Wen & Kesari, 2008).
4. Immunosuppressive Tumor Microenvironment
GBM creates a profoundly immunosuppressive microenvironment through:
- Myeloid-derived suppressor cells (MDSCs)
- Tumor-associated macrophages (TAMs)
- Regulatory T cells
- Cytokine-mediated immune suppression
This limits the effectiveness of immunotherapies that have shown success in other cancers.
5. Resistance to Standard Therapies
The current standard-of-care includes: Surgical resection, Radiation therapy, Temozolomide (TMZ); However, most patients eventually develop resistance, resulting in tumor recurrence.
Progression in GBM Therapeutics
Although GBM remains difficult to treat, major advances in molecular biology, immunotherapy, and translational oncology are reshaping the therapeutic landscape.
Standard-of-Care Therapies
Surgery: Maximal safe surgical resection remains the first-line intervention for newly diagnosed GBM. Surgery reduces tumor burden and relieves intracranial pressure but rarely eliminates all infiltrating cells.
Radiation Therapy: Radiotherapy is typically administered after surgery to target residual tumor cells.
Temozolomide (TMZ): Temozolomide is an oral alkylating chemotherapy agent commonly combined with radiation therapy. Patients with MGMT promoter methylation often show improved responses (Stupp et al., 2005).
Emerging Therapeutic Strategies for GBM
1. Targeted Therapies
Researchers are developing therapies targeting molecular abnormalities such as: EGFR inhibitors, VEGF inhibitors, PI3K/mTOR pathway inhibitors, and IDH inhibitors. However, clinical outcomes remain limited due to pathway redundancy and adaptive resistance mechanisms.
2. Immunotherapy
Immunotherapy has become a major focus in GBM research, although clinical success remains challenging due to the highly immunosuppressive tumor microenvironment. Immune checkpoint inhibitors targeting PD-1 and CTLA-4 have shown transformative outcomes in several cancer types but have demonstrated limited efficacy in GBM. In parallel, CAR-T cell therapies targeting antigens such as EGFRvIII, IL13Rα2, and HER2 are actively being investigated for their ability to selectively eliminate glioblastoma cells. Other emerging strategies include oncolytic virus therapy, which uses engineered viruses to infect and destroy tumor cells while stimulating antitumor immune responses.
Additionally, Natural Killer (NK) cell-based therapies are gaining attention as promising approaches because NK cells can recognize and eliminate tumor cells without prior antigen sensitization (Lim et al., 2018). NK therapeutics are being actively explored to enhance direct tumor cell killing, target glioma stem-like cells, and modulate the highly immunosuppressive GBM tumor microenvironment. Current approaches include allogeneic NK cell therapies, engineered NK cells, cytokine-activated NK platforms, and combination strategies with immune checkpoint inhibitors or other immunotherapies.

Lambda Biologics Solution: Modeling Glioblastoma Multiforme Using Human Cerebral Organoids
Human cerebral organoid-based GBM models are emerging as advanced preclinical platforms that more accurately replicate the structural and biological complexity of the human brain compared with conventional 2D cell cultures. By integrating patient-derived glioblastoma cells or introducing tumor-associated genetic alterations into cerebral organoids, researchers can generate physiologically relevant 3D models that mimic key hallmarks of GBM, including tumor invasion, intratumoral heterogeneity, glioma stem-like cell behavior, therapy resistance, and interactions with the tumor microenvironment (Hubert et al., 2016; Jacob et al., 2020)
At Lambda Biologics, we have developed a Glioblastoma Multiforme model using human cerebral organoids co-cultured with patient-derived GBM cells to support translational neuro-oncology research and therapeutic development. These advanced 3D platforms enable physiologically relevant evaluation of tumor progression, invasion, and therapeutic response while better preserving the heterogeneity and microenvironmental characteristics of human GBM.
Read more: Modeling Glioblastoma Multiforme Using Human Cerebral Organoids
Our organoid-based models are increasingly applied in drug screening, immunotherapy evaluation, biomarker discovery, and precision oncology studies, including NK cell and CAR-T therapeutic assessment. In addition, advanced co-culture systems incorporating immune cells, microglia, endothelial cells, and stromal components allow more comprehensive investigation of the highly immunosuppressive GBM microenvironment, including immune suppression, cytokine signaling, angiogenesis, and therapy-induced remodeling (Ravi et al., 2022). Compared with conventional 2D cultures, cerebral organoid models provide improved predictive value for clinical outcomes and support more human-relevant approaches for studying disease mechanisms, resistance pathways, and personalized therapeutic strategies (Jacob et al., 2020).
Conclusion
Glioblastoma Multiforme remains one of the most challenging cancers in modern oncology due to its aggressive biology, high heterogeneity, immune evasion, and therapeutic resistance. However, advances in immunotherapy, NK cell platforms such as CBT-101 NK, and human-relevant disease models are rapidly reshaping the GBM research landscape.
Human cerebral organoids are becoming powerful tools for studying tumor progression, invasion, tumor microenvironment interactions, and therapeutic response in more physiologically relevant settings. Combined with emerging technologies such as AI-driven drug discovery, multi-omics analysis, and advanced co-culture systems, these platforms may accelerate the development of more predictive and personalized therapeutic strategies for GBM patients.
Unlocking Human Insight with Organoid Models
Metabolic Diseases | Inflammation | Immunology | Respiratory Disease | Neuroscience | Gastrointestinal Disease





